Myelodysplastic syndromes (MDS) constitute a heterogeneous group of clonal hematopoietic stem cell disorders, characterized by ineffective hematopoiesis, peripheral cytopenias, and a risk of progression to acute leukemia. We report the results of a retrospective descriptive study of 100 MDS cases diagnosed at the hematology laboratory of HMIMV in Rabat over a 7-year period (January 2018 to December 2024), using a standardized data collection form for epidemiological, clinical, and biological data. The main objective of this work was to analyze the diagnostic contribution of bone marrow examination in MDS, specifying its indications and the main abnormalities observed. The mean age at diagnosis was 69 years (range: 41-93 years), with a moderate male predominance (sex ratio = 1.38). Clinically, anemic syndrome was the most frequent presenting manifestation (70%), followed by hemorrhagic manifestations (12%) and infectious manifestations (10%). Biological analysis revealed anemia in 90% of patients (mean hemoglobin: 9 g/dL), thrombocytopenia in 63% of cases, and leukopenia in 42% of cases. The anemia was normocytic in 55.6% of cases, macrocytic in 33.3%, and microcytic in 11.1%. Bone marrow examination revealed dyserythropoiesis in 92% of patients, dysgranulopoiesis in 65% of cases, and dysmegakaryopoiesis in 45% of cases. The median percentage of bone marrow blasts was 4.89%. According to the 2016 WHO classification, MDS-MLD were the most frequent (48%), followed by MDS-EB1 (21%) and MDS-EB2 (12%). The results of this study are consistent with national and international literature data, confirming the central role of bone marrow examination in MDS diagnosis and highlighting the importance of a multidisciplinary approach for optimal management of these complex hematological malignancies.
| Published in | European Journal of Clinical and Biomedical Sciences (Volume 12, Issue 2) |
| DOI | 10.11648/j.ejcbs.20261202.11 |
| Page(s) | 17-26 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Myelogram, Myelodyplastic Neoplasm, Diagnosis, WHO Classification
Study | Anemia (%) | Thrombocytopenia (%) | Neutropenia/Leucopenia (%) |
|---|---|---|---|
Our study | 90.0 | 63.0 | 42.0 |
Maaroufi et al. | 76.0 | 69.0 | 38.0 |
Baiza et al. | 96.0 | 44.0 | 35.0 |
Bernasconi et al. | 56.6 | 51.3 | 46.4 |
Massimo et al. | 41.0 | 31.0 | 36.0 |
MDS | Myelodisplastic Neoplasms |
WHO | World Health Organization |
HMIMV | Mohammed V Military Teaching Hospital |
CBC | Complete Blood Count |
MGG | May-Grünwald-Giemsa |
MDS-MLD | MDS with Multilineage Dysplasia |
MDS-SLD | MDS with Single-lineage Dysplasia |
MDS-EB 1 | MDS with Excess Blasts Type 1 |
MDS-EB 2 | MDS with Excess Blasts Type 2 |
MDS-RS-MLD | MDS with Ring Sideroblasts and Multilineage Dysplasia |
MDS-RS-SLD | MDS with Ring Sideroblasts and Single-lineage Dysplasia |
MDS-5q | MDS with Isolated Del (5q) |
MDS-U | MDS Unclassifiabl |
| [1] | Hajar S, Zahrae LF, Hicham Y, Mustapha AA, Mohamed C. The Role of Myelogram in Diagnosis of Malignant Hemopathies. Am J Lab Med. oct 2021; 6(5): 70‐6. |
| [2] | Krause H, Manz MG, Gerber B. Syndrome myelodysplasique: physiopathologie, diagnostic et traitement. Forum Medical Suisse ‒ Swiss Medical Forum [Internet]. 2013 [cited 16 juin 2025]; 13. Disponible sur: |
| [3] | Maaroufi HE, Ababou M, Hammani A, Ahchouch S, Jennane S, Mahtat M, et al. Prise en charge des syndromes myelodysplasiques au Maroc à propos d ́une etude mono- centrique. Pan Afr Med J. 2 dec. 2020; 37: 300. |
| [4] | Hanane M, Ilham K, Zahir H, Hicham Y, Mustapha AA, Mohammed C. Myelodysplastic Syndromes Experience of the Laboratory of the Military Hospital Avicenna Marrakech. Am J Lab Med. dec. 2019; 4(6): 115‐8. |
| [5] |
Masson E. EM-Consulte. [cite 2 juill. 2025]. Manifestations immunes associees aux syndromes myelodysplasiques. Etude prospective de 40 patients. Disponible sur:
https://www.em-consulte.com/article/37401/manifestations-immunes-associees-aux-syndromes-mye |
| [6] | Seguier J. Manifestations auto-immunes associees aux syndromes myelodysplasiques: description d’une cohorte regionale et revue de la litterature. 2017; |
| [7] | Troussard X, Malet M, Duchenet V, Mouchel D, Cheze S, Collignon A. Epidemiologie des syndromes myelodysplasiques (SMD) et des syndromes myelodysplasiques/syndromes myeloproliferatifs (SMD/SMP): Experience du Registre regional des hemopathies malignes de Basse-Normandie. Revue Francophone des Laboratoires. 1 juin 2009; 2009 [413]: 25‐9. |
| [8] | Bernasconi P, Klersy C, Boni M, Cavigliano PM, Calatroni S, Giardini I, et al. World Health Organization classification in combination with cytogenetic markers improves the prognostic stratification of patients with de novo primary myelodysplastic syndromes. Br J Haematol. mai 2007; 137(3): 193‐205. |
| [9] | Germing U, Strupp C, Kündgen A, Bowen D, Aul C, Haas R, et al. No increase in age-specific incidence of myelodysplastic syndromes. Haematologica. août 2004; 89(8): 905‐10. |
| [10] | Navarro I, Ruiz MA, Cabello A, Collado R, Ferrer R, Hueso J, et al. Classification and scoring systems in myelodysplastic syndromes: a retrospective analysis of 311 patients. Leuk Res. août 2006; 30(8): 971‐7. |
| [11] | Difference in clinical features between Japanese and German patients with refractory anemia in myelodysplastic syndromes - PubMed [Internet]. [cite 2 juill. 2025]. Disponible sur: |
| [12] | Mesli PN. Les syndromes myelodysplasiques en milieu hospitalier. |
| [13] | Baiza N, Bellamine K, Gamraoui k. Les syndromes myelodysplasiques: à propos de 45 cas. Hematologie. 2011; 17 [1]: 168. |
| [14] | Ma X, Does M, Raza A, Mayne ST. Myelodysplastic syndromes: incidence and survival in the United States. Cancer. 15 avr. 2007; 109(8): 1536‐42. |
| [15] | Dinmohamed AG, Visser O, van Norden Y, Huijgens PC, Sonneveld P, van de Loosdrecht AA, et al. Trends in incidence, initial treatment and survival of myelodysplastic syndromes: a population-based study of 5144 patients diagnosed in the Netherlands from 2001 to 2010. Eur J Cancer. mars 2014; 50(5): 1004‐12. |
| [16] | Ehsan A, Aziz M. Clinico-haematological characteristics in Pakistani patients of primary myelodysplastic syndrome according to World Health Organization classification. J Coll Physicians Surg Pak. avr. 2010; 20 [4]: 232‐6. |
| [17] | Samba Diago N. Aspects cytologiques des syndromes myelodysplasiques au Senegal. Science Lib Editions Marsenne. 2009; 2 (90902). |
| [18] | Ben Amor I, Mnif H, Kassar O, Bouaziz H, Rekik H, Mseddi S et al. Immunisation anti-erythrocytaire dans les syndromes myelodysplasiques: etude à propos de 53 patient. |
| [19] | Ndiaye Fatou, Samba Diego, Toure-Fall Awa Oumar, Fall Seynabou, Ka Mamadou Mourtalla, Moreira-Diop Therèse. Aspects cytologiques des syndromes myelodysplasiques au Senegal: etude retrospective de 13 patients. Science Lib Editions Mersenne. 2009; Volume 2(N° 090902). |
| [20] |
Syndromes myelodysplasiques et leucemies secondaires: generalites, diagnostic et classification - EM consulte [Internet]. [cite 2 juill. 2025]. Disponible sur:
https://www.em-consulte.com/article/1435036/syndromes-myelodysplasiques-et-leucemies-secondair |
| [21] | Myelodysplastic syndromes in Thailand: a retrospective pathologic and clinical analysis of 117 cases - PubMed [Internet]. [cite 2 juill. 2025]. Disponible sur: |
| [22] |
Groupe Francophone des Myélodysplasies, “Référentiel SMD du GFM Octobre 2008”. Available from:
http://www.gfmgroup.org/fichiers/recommandations/recommandation_20081114170733.pdf |
| [23] | Les syndromes myelodylasiques (A propos de 34 cas) [Internet]. [cite 2 juill. 2025]. Disponible sur: |
| [24] | Hmissi B, Gouider E, Ben Salah N, El Borgi W, Besbes S et al. Profil epidemiologique, cytologique des syndromes myelodysplasiques: experience de l ́hopital Aziza Othmana. |
APA Style
Hamza, A., Arwa, B., Youssef, L., Youssef, D., Ilham, O., et al. (2026). The Role of Myelogram in the Diagnosis of Myelodysplastic Neoplasms. European Journal of Clinical and Biomedical Sciences, 12(2), 17-26. https://doi.org/10.11648/j.ejcbs.20261202.11
ACS Style
Hamza, A.; Arwa, B.; Youssef, L.; Youssef, D.; Ilham, O., et al. The Role of Myelogram in the Diagnosis of Myelodysplastic Neoplasms. Eur. J. Clin. Biomed. Sci. 2026, 12(2), 17-26. doi: 10.11648/j.ejcbs.20261202.11
@article{10.11648/j.ejcbs.20261202.11,
author = {Arrama Hamza and Bouchara Arwa and Loubadi Youssef and Dakki Youssef and Orchi Ilham and Essahli Khadija and Kahouli Sophia and Zahid Hafid},
title = {The Role of Myelogram in the Diagnosis of Myelodysplastic Neoplasms},
journal = {European Journal of Clinical and Biomedical Sciences},
volume = {12},
number = {2},
pages = {17-26},
doi = {10.11648/j.ejcbs.20261202.11},
url = {https://doi.org/10.11648/j.ejcbs.20261202.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ejcbs.20261202.11},
abstract = {Myelodysplastic syndromes (MDS) constitute a heterogeneous group of clonal hematopoietic stem cell disorders, characterized by ineffective hematopoiesis, peripheral cytopenias, and a risk of progression to acute leukemia. We report the results of a retrospective descriptive study of 100 MDS cases diagnosed at the hematology laboratory of HMIMV in Rabat over a 7-year period (January 2018 to December 2024), using a standardized data collection form for epidemiological, clinical, and biological data. The main objective of this work was to analyze the diagnostic contribution of bone marrow examination in MDS, specifying its indications and the main abnormalities observed. The mean age at diagnosis was 69 years (range: 41-93 years), with a moderate male predominance (sex ratio = 1.38). Clinically, anemic syndrome was the most frequent presenting manifestation (70%), followed by hemorrhagic manifestations (12%) and infectious manifestations (10%). Biological analysis revealed anemia in 90% of patients (mean hemoglobin: 9 g/dL), thrombocytopenia in 63% of cases, and leukopenia in 42% of cases. The anemia was normocytic in 55.6% of cases, macrocytic in 33.3%, and microcytic in 11.1%. Bone marrow examination revealed dyserythropoiesis in 92% of patients, dysgranulopoiesis in 65% of cases, and dysmegakaryopoiesis in 45% of cases. The median percentage of bone marrow blasts was 4.89%. According to the 2016 WHO classification, MDS-MLD were the most frequent (48%), followed by MDS-EB1 (21%) and MDS-EB2 (12%). The results of this study are consistent with national and international literature data, confirming the central role of bone marrow examination in MDS diagnosis and highlighting the importance of a multidisciplinary approach for optimal management of these complex hematological malignancies.},
year = {2026}
}
TY - JOUR T1 - The Role of Myelogram in the Diagnosis of Myelodysplastic Neoplasms AU - Arrama Hamza AU - Bouchara Arwa AU - Loubadi Youssef AU - Dakki Youssef AU - Orchi Ilham AU - Essahli Khadija AU - Kahouli Sophia AU - Zahid Hafid Y1 - 2026/03/23 PY - 2026 N1 - https://doi.org/10.11648/j.ejcbs.20261202.11 DO - 10.11648/j.ejcbs.20261202.11 T2 - European Journal of Clinical and Biomedical Sciences JF - European Journal of Clinical and Biomedical Sciences JO - European Journal of Clinical and Biomedical Sciences SP - 17 EP - 26 PB - Science Publishing Group SN - 2575-5005 UR - https://doi.org/10.11648/j.ejcbs.20261202.11 AB - Myelodysplastic syndromes (MDS) constitute a heterogeneous group of clonal hematopoietic stem cell disorders, characterized by ineffective hematopoiesis, peripheral cytopenias, and a risk of progression to acute leukemia. We report the results of a retrospective descriptive study of 100 MDS cases diagnosed at the hematology laboratory of HMIMV in Rabat over a 7-year period (January 2018 to December 2024), using a standardized data collection form for epidemiological, clinical, and biological data. The main objective of this work was to analyze the diagnostic contribution of bone marrow examination in MDS, specifying its indications and the main abnormalities observed. The mean age at diagnosis was 69 years (range: 41-93 years), with a moderate male predominance (sex ratio = 1.38). Clinically, anemic syndrome was the most frequent presenting manifestation (70%), followed by hemorrhagic manifestations (12%) and infectious manifestations (10%). Biological analysis revealed anemia in 90% of patients (mean hemoglobin: 9 g/dL), thrombocytopenia in 63% of cases, and leukopenia in 42% of cases. The anemia was normocytic in 55.6% of cases, macrocytic in 33.3%, and microcytic in 11.1%. Bone marrow examination revealed dyserythropoiesis in 92% of patients, dysgranulopoiesis in 65% of cases, and dysmegakaryopoiesis in 45% of cases. The median percentage of bone marrow blasts was 4.89%. According to the 2016 WHO classification, MDS-MLD were the most frequent (48%), followed by MDS-EB1 (21%) and MDS-EB2 (12%). The results of this study are consistent with national and international literature data, confirming the central role of bone marrow examination in MDS diagnosis and highlighting the importance of a multidisciplinary approach for optimal management of these complex hematological malignancies. VL - 12 IS - 2 ER -
Hematology and Immunohematology Laboratory, Mohammed V Military Teaching Hospital, Rabat, Morocco;Faculty of Medicine and Pharmacy of Rabat, Mohammed V University of Rabat, Rabat, Morocco
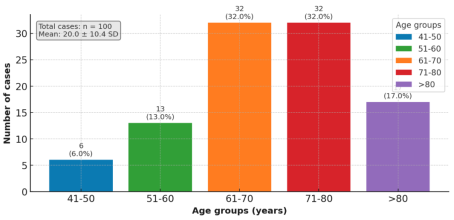
Figure 1. Distribution of MDS cases according to age.
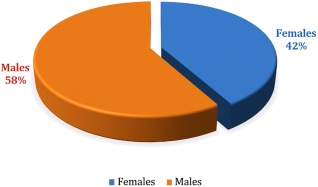
Figure 2. Distribution of MDS cases according to sex (N=100).
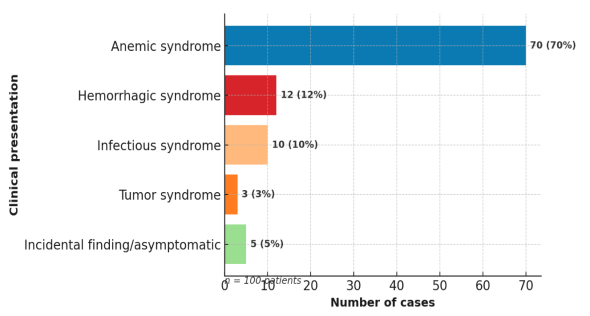
Figure 3. Distribution of clinical indications of myelogram.
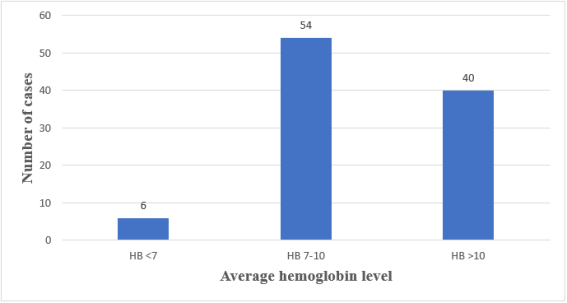
Figure 4. Distribution of MDS cases according to hemoglobin levels (N=100).
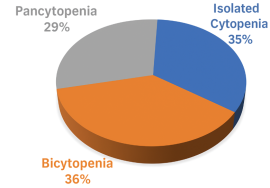
Figure 5. Distribution of MDS according to the presence of one or more peripheral cytopenias (N=100).
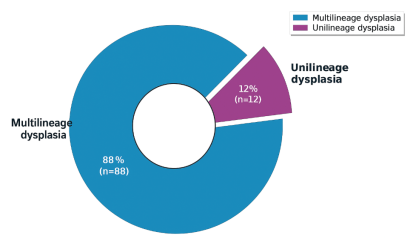
Figure 6. Distribution of MDS According to the Type of Dysplasia Observed.
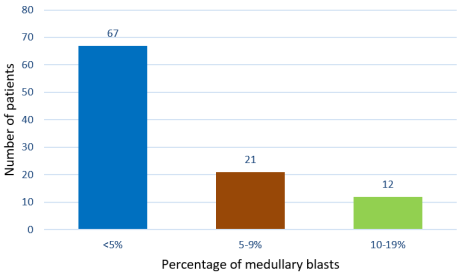
Figure 7. Distribution of MDS According to Bone Marrow Blast Percentage.
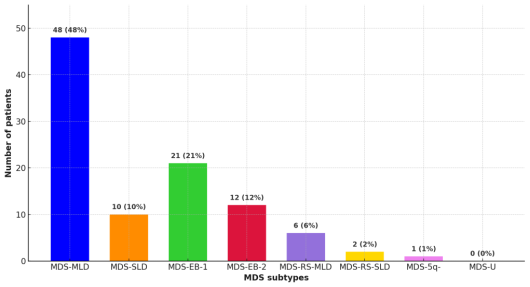
Figure 8. Distribution According to the 2016 WHO Classification.
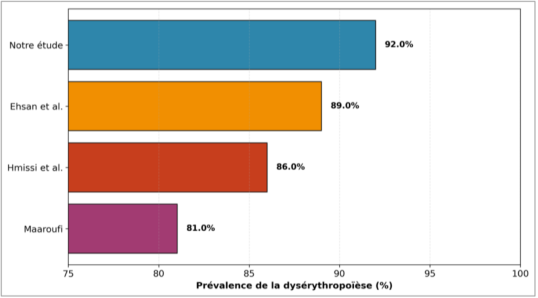
Figure 9. Dyserythropoïesis, most frequent morphological abnormality in MDS: comparison between different studies.

